
Too many pills, too many interactions
“You have to be really, really strategic about how you prescribe medications, because you might be worsening other things in the long run or the short run,”
 Said Jonathan Watanabe, chair of the Department of Clinical Pharmacy at the University of California at San Francisco.. Dr Watanabe is an expert in the field of geriatric prescribing. First of all, he warns about seniors getting drugs that may have negative interactions. Second of all, it might lead to a senior taking a medicine longer than the prescriber intended. “It gets sort of stuck on their patient profile in perpetuity,” said the Doctor.
Said Jonathan Watanabe, chair of the Department of Clinical Pharmacy at the University of California at San Francisco.. Dr Watanabe is an expert in the field of geriatric prescribing. First of all, he warns about seniors getting drugs that may have negative interactions. Second of all, it might lead to a senior taking a medicine longer than the prescriber intended. “It gets sort of stuck on their patient profile in perpetuity,” said the Doctor.
The dangers from the problem of polypharmacy are well recognized. The American Geriatrics Society has set created a “benchmark” for being able to safely prescribe senior’s medication.Doctors, nurses and other health care proffesionals ought to be more ccareful when it comes to “medication reconciliation,”. Yes, this means checking every medication a patient takes. An update medication list is a must. Yet overprescribing and the harms it causes persist, researchers have found. Providers may know about over-the-counter-pills, vitamins or other supplements which can make things worse.
“Care transitions, say from a nursing home to a hospital or vice versa, are high risk times for many reasons, and risks multiply because the two settings use totally different electronic record systems”
,Alice Bonner, a PA has worked on national models for safe prescribing. It gets even more challenging if the patient’s first language is not English. “
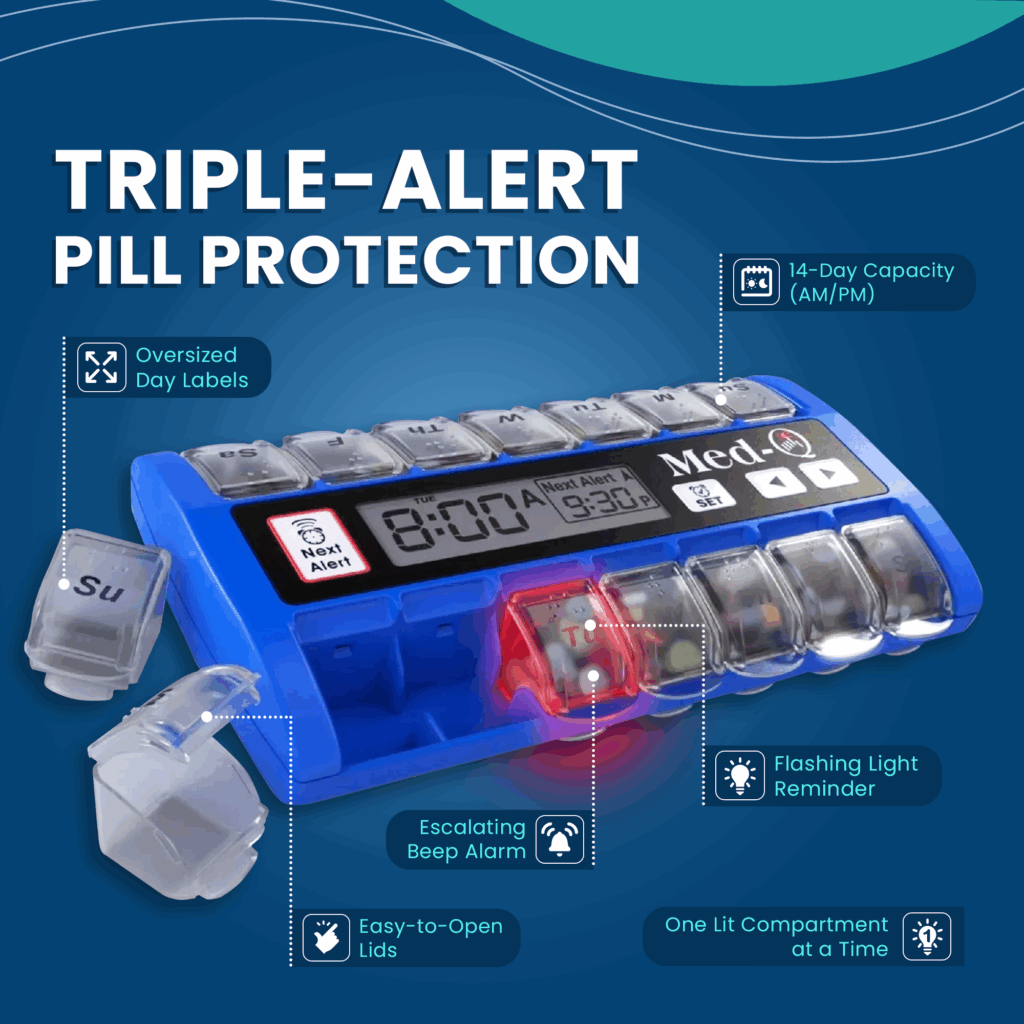
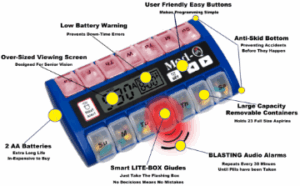 The first question, are they able to take their medications as prescribed by their healthcare proffesional? Is their regimen too complicated? Does it need to be simplified? Do the need a digital pill box with alarms that reminds and guides
The first question, are they able to take their medications as prescribed by their healthcare proffesional? Is their regimen too complicated? Does it need to be simplified? Do the need a digital pill box with alarms that reminds and guides
Other questions need to be answered. For example, they understand why it is being doesed that way? Many times patients don’t realize their Lasix is just a brand name. This pill is prescribed for congestive heart failure. They do not know that it is the same thing as furosemide. Many will wind up taking both the genirica nad name brand. the generic, they might end up taking both.
Medication reconciliation
Ideally, health providers do undertake “medication reconciliation. This is the term for, ” to figure out what’s helpful and what’s not” . Using modern techoligy is the key. Everything from a computerized medication list to a medication reminder with built in alalrms needs to be used. That’s what helps senior stay healthier and witha bertter Quiality of life. Bu it doesn’t always happen. And even in a top-notch system or home caregivers, things are often missed.
“People accrue medicines, right? Especially if they’re seeing multiple providers, that medicine list just grows,” said Susan Parks, director of geriatric medicine at Thomas Jefferson University in Philadelphia. Patients there are given a marked brown bag to bring in everything they take, prescription and non, so it can all be assessed. Some drugs are “deprescribed,” with explanation and reassurance that the patient is better without them. And sometimes patients and providers weigh trade-offs. For instance, a patient might want to stay on a drug for incontinence despite some chance of dizziness or confusion. And providers can then help minimize risks.

